Treatment for Chronic Neck Pain
The most common single basis for neck pain following injury and including whiplash are the neck (cervical) facet joints; they account for over 50% of patients with chronic neck pain after whiplash.
The two most common sources are the C2-3 and C5-6 Joints.
Pain generated from at the C2-3 segment is commonly felt as neck pain with headache (Cervicogenic headache). The C2-3 joint is the most common source of pain in individuals with chronic upper neck pain and cervicogenic headache.
Characteristics of Cervicogenic Headaches are
Unilateral and starts in the neck includes any 3 of the following:
- Pain triggered by movement, posture, pressure
- Ipsilateral neck, shoulder, arm pain
- Diminished range of movement
- Pain may be intermittent or fluctuating constantly
- Pain is moderate and non-throbbing
- Post traumatic in onset
Diagnosis of Cervicogenic Headache
To confirm a diagnosis of Cervicogenic headache generated by the C2-3 facet joint, is by an injection of local anaesthetic to the nerve supply of the affected joint – called a medial branch block (MBB).
Treatment of Cervicogenic Headache
By confirming a joint is the source of pain, treatment by radio frequency neurotomy (RF) will ensure a complete relief of pain in 86% of patients for 9-15 months
- the procedure can be repeated if necessary
- Injection of local anaesthetic into the cervical intra articular joints lacks accuracy; and injection of steroid into cervical facet joints lacks efficacy
Diagnosis of lower neck, trapezius, scapula and inter scapula pain following trauma including whiplash
By completing the diagnostic local anaesthetic injection (medial branch block), the facet joints can be confirmed or excluded as sources of pain.
Radio frequency neurotomy is a successful treatment for neck and shoulder pain, derived from the lower cervical facet joints.
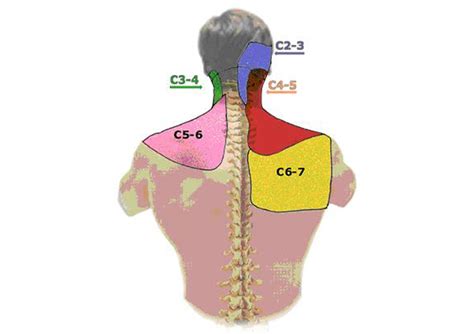
Diagram of Cervical Facet Joints: